Full Mouth Rehabilitation, Rebuilding Structure, Function, Occlusion, and Aesthetics Across Every Tooth
- Full Mouth Rehabilitation is the comprehensive restoration of every tooth, or every functional site where a tooth should be, across one or both dental arches.
It is the category of dentistry that re-engineers four things at once: structure, function, occlusion, and aesthetics, all against the background of periodontal and systemic health.

Full-Arch Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Immediate Load
Full-arch or multiple implant cases where provisional teeth are placed shortly after surgery in suitable clinical conditions.

Multiple Implant Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.

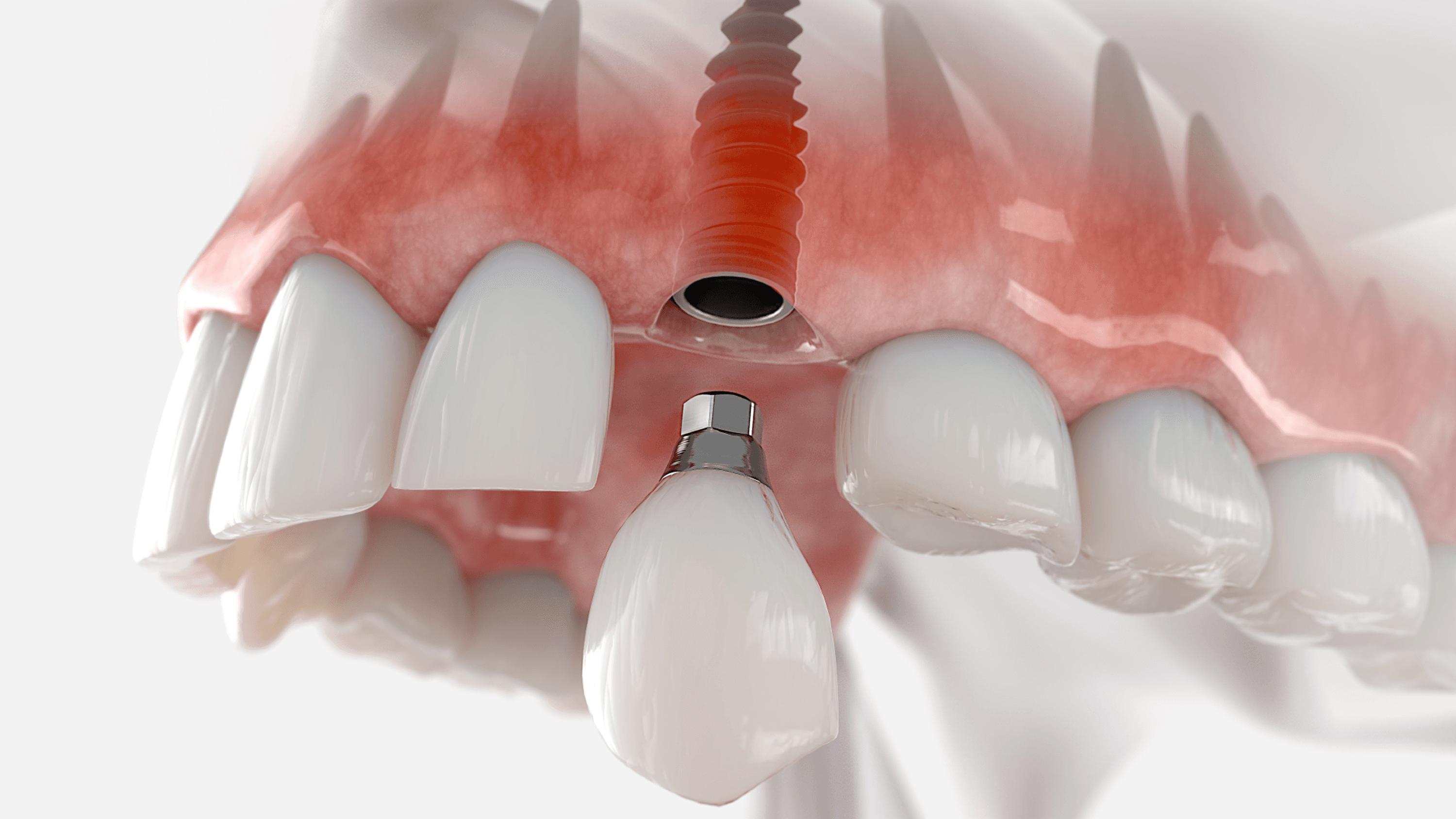
Single Tooth Implant
Single-tooth replacement with an implant and crown for a natural-looking, long-lasting result.

Bone Grafting & Advanced Surgical Support
Regenerative procedures performed to establish adequate bone volume for stable implant placement.

Revision & Complex Implant Cases
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Overview
Full Mouth Rehabilitation is the comprehensive restoration of every tooth, or every functional site where a tooth should be, across one or both dental arches. It is the category of dentistry that re-engineers four things at once: structure, function, occlusion, and aesthetics, all against the background of periodontal and systemic health.
Full Mouth Rehabilitation is the most demanding category of restorative dentistry, built on nearly a century of peer-reviewed functional-occlusion research, Dawson, Kois, Pankey, Hobo and Takayama, and delivered today with digital tools those same clinicians would have considered science fiction.
For patients reading from the UK
The Full Mouth Rehabilitation pathway available here is the same rehabilitation category practised by consultant prosthodontists on Harley Street, in Edinburgh, Manchester, Birmingham, Cardiff, and Belfast. The diagnostic frameworks (Dawson, Kois, Pankey), the occlusal principles (centric relation, anterior guidance, canine-protected occlusion), the implant protocols (All-on-4, All-on-6, zygomatic), and the material standards (monolithic zirconia, lithium disilicate, PEKK) are internationally consistent. What changes when you travel to Stunning Dentistry is not the clinical protocol, it is the specialist bench depth, the in-house digital infrastructure, and the total cost. We walk through exactly how that comparison lines up further down this page.
At Stunning Dentistry
Every Full Mouth Rehabilitation case carries a dual-clinician sign-off: Dr. Priyank Sethi and one senior consultant prosthodontist review and countersign the treatment plan before any irreversible step begins. That dual-signature protocol is the single most important safeguard in comprehensive dentistry, because once you cross the line from a ten-unit case into a full-arch reconstruction, there is no solo-clinician shortcut that ages well. The protocol is named SD-FMR-05 and it runs on every case in every location we operate.
Questions about this procedure?
What Full Mouth Rehabilitation Actually Means
Full Mouth Rehabilitation, abbreviated here as FMR, is the simultaneous or sequentially staged restoration of:
- Every remaining tooth that can be preserved, restored to functional form and load-bearing ability
- Every missing tooth site replaced by an implant, bridge unit, or removable prosthesis component
- The occlusal scheme that governs how the upper and lower arches meet, glide, and protect one another
- The vertical dimension of occlusion (VDO) that determines facial height, lip support, and jaw-muscle balance
- The periodontal foundation that has to carry whatever we build on top of it
- The aesthetic outcome, smile line, incisal display, buccal corridor, lip dynamics
What Full Mouth Rehabilitation Is Not
- It is not "a lot of crowns." It is a redesigned bite.
- It is not a cosmetic procedure. Aesthetics are one of four outputs, not the driver.
- It is not a single-visit decision. The diagnostic phase alone takes between two and six weeks.
- It is not something any general dentist should undertake alone. A genuine FMR case needs at least three GDC-registered specialists reading the same diagnostic file.
- It is not a "veneer package." The All-Ceramic 28-unit makeover marketed on Instagram is, nine times in ten, a crown-and-veneer reconstruction dressed up as FMR without the diagnostic backbone.
The Four Outputs of a Correctly Delivered FMR
4. Aesthetic restoration, the smile reads as natural, age-appropriate, and structurally coherent with the face.
At Stunning Dentistry
We hold the line on the four-output definition because the industry does not. We have had patients fly in with prior "full mouth makeovers" completed elsewhere where the aesthetic was acceptable but the occlusal scheme was never designed, the anterior guidance was shallow, the posteriors were in constant interference, and the restorations began fracturing within eighteen months. Rebuilding a bite that was never engineered in the first place is harder than rebuilding one that was lost to wear. That is why we insist on SD-FMR-05.
Ready to discuss your options?
When Full Mouth Rehabilitation Is Indicated
FMR is indicated when one or more of the following clinical pictures is present across both arches or across a single arch that cannot be treated in isolation.
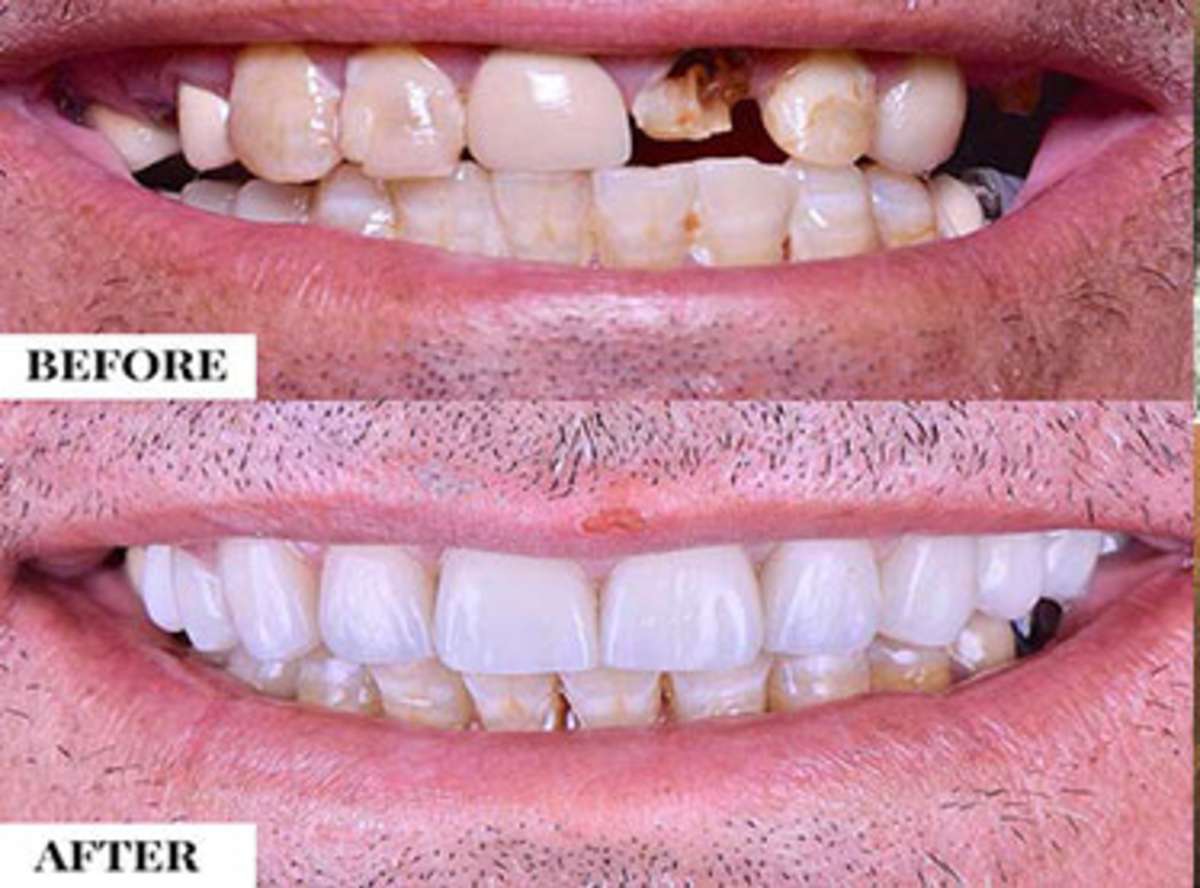
Severe Tooth Wear
End-Stage Periodontitis
Failed Large Restorations
Congenital Conditions
- Amelogenesis imperfecta, defective enamel formation leaves teeth structurally weak from eruption. Most patients need FMR by their late twenties or thirties.
- Dentinogenesis imperfecta, the underlying dentine is compromised; rehabilitation sequence differs from AI.
- Ectodermal dysplasia, hypodontia plus conical teeth plus compromised soft tissue, often requiring implant-supported solutions from adulthood onward.
- Severe hypodontia, six or more congenitally missing teeth change the restorative geometry sufficiently that piecemeal treatment will not hold.
Trauma
Failed Prior Rehabilitation
Psychogenic Bruxism and Severe Parafunction
When nocturnal or daytime parafunction generates forces capable of fracturing natural tooth structure, any FMR has to be engineered around those forces, not merely protected from them. This means material choices (monolithic zirconia over layered ceramic), occlusal design (steeper or shallower anterior guidance depending on the muscle pattern), and splint therapy that begins before restoration and continues indefinitely afterward.
At Stunning Dentistry
We record a formal BEWE score, a periodontal chart, a full-mouth series of radiographs, and a T-Scan digital occlusal map at the first diagnostic visit. No FMR plan is written before those four data sets exist in the patient's file. It is slower than quoting from a photograph; it is also the only way to quote something that will still be true in ten years.
Curious about costs and timelines?

The Diagnostic Frameworks That Guide Every Case
FMR is not performed by intuition. Four internationally validated diagnostic frameworks govern how we read a case, and every Stunning Dentistry FMR file documents against at least two of them.
The Kois Framework
The Dawson Framework
The Pankey Philosophy
The Hobo and Takayama Twin-Stage Method
Hobo and Takayama's twin-stage procedure engineers the occlusion in two distinct steps: first, a cusp-to-fossa form that establishes stable centric contacts; second, an anterior guidance refinement that disoccludes the posteriors during excursive movements. The method is mathematical, specific disclusion angles calibrated per case, and it is particularly powerful when the prior occlusion has collapsed and no historical guidance remains to copy.
At Stunning Dentistry
The four frameworks are not competing schools; they are complementary lenses. Kois tells us where the risk sits. Dawson tells us where the bite should be. Pankey tells us when to stop and show the patient. Hobo and Takayama tell us how to cut the ceramic. Every FMR file documents the Kois risk scores in the opening diagnosis, the Dawson centric relation record in the functional records, the Pankey approval gate dates in the consent log, and the Hobo disclusion angles in the prosthetic prescription. If your FMR plan elsewhere does not reference at least two of the four, the plan has been written from photographs alone.
Want a personalised treatment plan?

Core Occlusal Concepts You Need to Understand
If you are going to commit tens of thousands of pounds to rebuilding your bite, you deserve to understand the vocabulary. Here are the concepts we will use in your plan.
Vertical Dimension of Occlusion (VDO)
Centric Relation (CR) and Maximum Intercuspation (MIP)
The Posselt Envelope
Anterior Guidance
Canine-Protected Occlusion vs Group Function
The Christensen Phenomenon
The Envelope of Parafunction
The boundary of jaw motion during bruxism, clenching, and other non-functional activity. The envelope of parafunction extends beyond the envelope of function, and FMR materials and designs have to survive both.
At Stunning Dentistry
Every patient's diagnostic workup produces a written occlusal design brief before any restorative work begins. It names the target VDO in millimetres, the CR-MIP slide to be closed, the anterior guidance angle, and the canine-protected-versus-group-function decision. That brief is countersigned by two consultant prosthodontists under SD-FMR-05. If you have ever received a treatment plan that does not contain those four data points, the plan was not a rehabilitation plan.
Questions about this procedure?

The Five Modalities of Full Mouth Rehabilitation
FMR is not a single procedure. It is a selection decision across five modalities, each with distinct biological demands, timelines, costs, and long-term outcomes. The rest of this page, and the downstream procedure pages linked from it, walks through each one in depth.
A sixth pathway, staged orthodontic plus restorative, is not a modality in itself but a preparation protocol that reshapes the dental arches before any restorative modality is chosen. Alistair's case, profiled later, is the archetype.
At Stunning Dentistry
We run all six pathways in-house under one governance structure. The decision about which modality is right for you is taken in the diagnostic phase by a three-specialist panel: consultant prosthodontist, consultant periodontist, and the oral surgeon who would perform any implant placement. No modality is selected because it is the most profitable or the quickest to deliver. The modality is selected because the bone, the bite, and the biology say so.
Ready to discuss your options?
All-on-4 Full-Arch Fixed
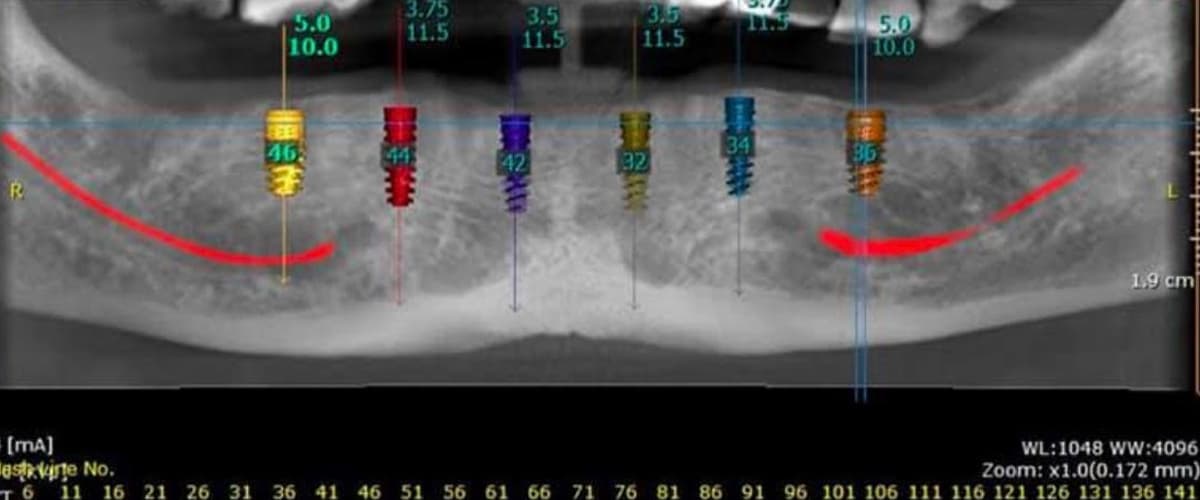
All-on-4 is the most widely validated full-arch fixed implant protocol in the world. Four implants per arch, two axial in the anterior, two tilted posterior to bypass the maxillary sinus or the mandibular inferior alveolar nerve, support a screw-retained bridge delivered as a provisional on the day of surgery and as a definitive zirconia prosthesis three to six months later.
That page runs through the biomechanics of tilted implants, the immediate-loading protocol, the provisional-to-definitive transition, the comparison with All-on-6 and conventional implant protocols, the cost band in GBP, and the three-trip UK patient journey in depth.
At Stunning Dentistry
When we quote All-on-4, we quote the protocol Paulo Maló originated and the one his published data covers. Not a four-implant approximation with axial-only placement. Not a "budget full arch" with third-party implants that do not have the ten-year survival data to back them up. The implants are Nobel Biocare or Straumann. The prosthesis is a milled titanium framework with a 4Y-TZP multilayer zirconia overlay (900 MPa flexural strength). The clinical protocol is audited against SD-FMR-05. That is what All-on-4 is.
Curious about costs and timelines?

All-on-6 When Bone Allows
All-on-6 adds two implants to the All-on-4 design, providing a shorter cantilever, broader load distribution, and a reserve of anchorage for patients with high bite force, large arches, or a history of parafunction. It requires more bone than All-on-4, two additional implant sites have to be genuinely placeable without grafting, so candidacy is stricter.
That page covers the candidacy criteria, the biomechanical case for six implants over four, the Jensen classification for full-arch implant design, the ten-year survival data, the material choices, the UK cost comparison, and the multi-trip journey in detail.
At Stunning Dentistry
We recommend All-on-6 over All-on-4 in roughly one in three of our full-arch mandibular cases, and in a smaller proportion of maxillary cases. The decision is made on CBCT bone volume analysis, measured bite force (we use a T-Scan bite-force record at diagnostic workup), and parafunction history. If All-on-4 is clinically adequate, we do not add two implants to increase the invoice. If it is not, we do not cut corners to hit a round number.
Want a personalised treatment plan?
Zygomatic When Bone Is Gone
Zygomatic implants anchor into the zygomatic bone, the cheekbone, bypassing a maxilla that has resorbed beyond the volume required for conventional or tilted placement. Originally developed by Professor Per-Ingvar Brånemark for oncologic maxillary reconstruction in the 1990s, zygomatic implants have become the standard answer for the severely atrophic maxilla and for the revision of failed maxillary full-arch cases.
That page covers the ZAGA classification for zygomatic-alveolar anatomy, the quad vs hybrid decision, the surgical approach, the sinus management protocol, the published data, the UK specialist landscape, and the GBP cost comparison.
At Stunning Dentistry
Zygomatic cases are performed only at our Hyderabad flagship and only by surgeons with documented zygomatic training and at least 150 lifetime cases. We will not take on a zygomatic case at a location without that exact capability. If your anatomy sits in the grey zone between severe atrophy and true zygomatic indication, we will tell you, and where appropriate we will recommend a staged approach (sinus augmentation, conventional tilted implants) that stays within the safer clinical envelope.
Questions about this procedure?

Teeth-in-a-Day Same-Day Fixed
"Teeth-in-a-Day" is the patient-facing name for the immediate-loading protocol that delivers a screw-retained provisional full-arch bridge on the same day the implants are placed. It is not a distinct surgical technique, the underlying implant design is most often All-on-4 or All-on-6, but the workflow, the same-day fabrication infrastructure, and the primary-stability thresholds that qualify a patient are specific enough to warrant their own page.
That page details the immediate-loading literature, the primary-stability thresholds, the in-house same-day lab workflow (3D printing, chairside milling), the honest conversion rates (what proportion of patients actually achieve same-day fixed teeth), and the UK patient journey.
At Stunning Dentistry
Our published same-day fixed-teeth conversion rate for FMR candidates is 86 per cent. The remaining 14 per cent are delayed-loaded because the intraoperative primary-stability data did not justify loading. We publish the figure rather than promise 100 per cent because the 100 per cent promise is what goes wrong in this category. Immediate loading is an honest-stability decision, not a marketing commitment.
Ready to discuss your options?
Smile Design for Aesthetic-Led Cases
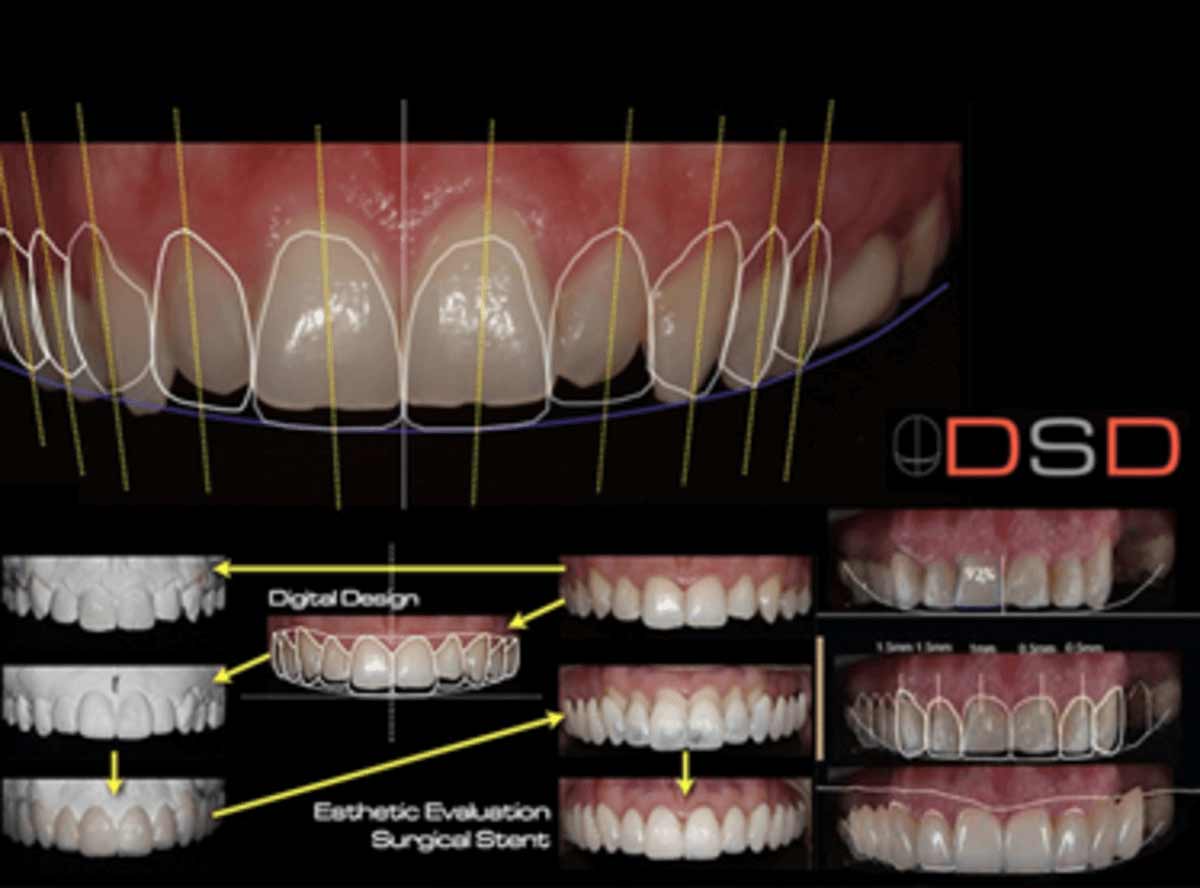
Some FMR cases are aesthetic-led: the function is substantially intact, the occlusion is stable, but the appearance of the dentition has deteriorated to the point where the patient is no longer comfortable in their own face. These cases are approached through Digital Smile Design, a protocol that integrates facial photographs, video analysis, intraoral scans, and phonetic testing into a complete aesthetic and functional preview before any tooth is prepared.
That page covers the DSD workflow, the 2D-to-3D mock-up process, the PMMA try-in phase, the material ladder (lithium disilicate veneers through monolithic zirconia crowns), the phonetic and lip-dynamic testing, and the UK cost comparison for aesthetic-led cases.
At Stunning Dentistry
We run DSD through a combination of Zirkonzahn PlanOral and 3Shape Dental System. The mock-up is reviewed on a high-resolution 2D print, then printed in wax, then trial-fitted in PMMA, then translated into the definitive material. Three patient approval gates before the first definitive unit is cemented. No patient has ever left our chair with a definitive set of units they have not seen and approved in PMMA first.
Curious about costs and timelines?
Full Mouth Tooth-Supported Rehabilitation
When the dentition is structurally preservable, BEWE scores severe enough to justify intervention, but root lengths, periodontal support, and crown-to-root ratios still viable, tooth-supported FMR rebuilds the full arch on the existing teeth. Typically 28 units of crowns, onlays, and veneers, fabricated from monolithic zirconia or lithium disilicate (IPS e.max or Vita Suprinity), planned at an increased VDO to recover lost vertical dimension, and sequenced to preserve the patient's comfort and function throughout.
Graham's case, profiled later, is a staged mixed-modality example: tooth-supported FMR on the lower arch (e.max and 4Y-TZP), All-on-4 on the upper arch where the BEWE damage was beyond preservable.
At Stunning Dentistry
We do not push every FMR candidate toward implants. Roughly 30 per cent of our UK FMR cases are tooth-supported or partially tooth-supported. The cost of a tooth-supported FMR is often within 15 per cent of an implant-supported FMR at our pricing, and the biological calculation, preserved periodontal ligament, no surgical morbidity, no osseointegration risk, can favour the tooth-supported route. That is a clinical decision, not a budget decision.
Want a personalised treatment plan?
Hybrid Implant-and-Tooth, and Why We Avoid It
A bridge that spans natural teeth and implants on the same prosthesis, a hybrid restoration, has been an attempted modality for decades. We avoid it, and most contemporary prosthodontic evidence supports that position.
There are narrow exceptions: non-rigid connectors with documented periodontal health and strict occlusal design; specific salvage scenarios where the tooth-plus-implant bridge is a time-limited bridge to a future all-implant plan. Outside those exceptions, we plan around the mismatch, either all-tooth-supported, or all-implant-supported, not both in one rigid unit.
At Stunning Dentistry
We will not plan a rigid tooth-plus-implant rehabilitation as a long-term solution. If your existing bridgework is this design and is still working, we will not reflexively replace it, but we will not build a new one. The biomechanics have been debated in the literature since 1995 and the consensus now is clear enough to act on.
Questions about this procedure?

Implant Overdentures and Combination Cases
An implant overdenture is a removable prosthesis retained by two to four implants via bar, Locator, or ball attachments. It sits between a conventional denture (unstable, palate-covered, retained by suction alone) and a fixed full-arch implant restoration (screw-retained, non-removable, palate-free). For a subset of patients, severe bone resorption incompatible with fixed restoration budget, finger dexterity limitations that favour removability for hygiene access, or conservative transition cases, it is the right answer.
Combination cases, one arch fixed, one arch removable, are a recognised and appropriate modality when bone, budget, or biology makes symmetric fixed restoration impossible. A lower fixed All-on-4 against an upper implant overdenture, for instance, restores function across the full mouth while matching the biology of each arch. The opposite combination (upper fixed, lower overdenture) is rarer because lower dentures are inherently less stable.
At Stunning Dentistry
We treat overdentures as a legitimate clinical modality, not a budget concession. We quote them honestly, sequence them properly, and document the service-life expectations up front. A well-made overdenture is a better answer than a compromised fixed case, every time.
Ready to discuss your options?

The Interdisciplinary Team, Who Does What
No single clinician delivers a genuine FMR. The minimum team is three GDC-registered specialists; the typical team is five to seven. Here is the role map we run against.
Consultant Prosthodontist
Consultant Periodontist
Oral Surgeon or Specialist in Oral Surgery
Endodontist
Orthodontist
TMJ and Occlusion Specialist
Dental Laboratory Technician
Fabricates the provisionals and definitives. At Stunning Dentistry our laboratory is fully in-house: Zirkonzahn PlanOral virtual articulator, Roland milling units, Formlabs 3D printers, sintering ovens in dedicated rooms. The technician is present at the PMMA try-in and the definitive seating. External-lab dependencies create communication gaps that age poorly in FMR cases.
At Stunning Dentistry
The interdisciplinary team is not a brochure; it is a rota. Every FMR case is presented at a Tuesday-morning case conference attended by the prosthodontist, the periodontist, the oral surgeon, and where relevant the endodontist and orthodontist. The plan that goes into the patient's file is the plan that survives that meeting. No solo sign-off on an FMR, ever.
Curious about costs and timelines?
The Digital Workflow, 2025 to 2026 Standard
The 2025 to 2026 FMR digital workflow is genuinely different from what was possible even five years ago. Here is what it looks like at Stunning Dentistry.
Intraoral Scanning
Cone Beam CT (CBCT)
Digital Smile Design (DSD)
Virtual Articulator
CAD-CAM Design and Fabrication
Three-Stage Patient Approval Gate (SD-FMR-05)
3. Definitive approval, the patient reviews the definitive units at try-in (before any cementation or screw torque), confirms aesthetics, phonetics, and bite, and only then is the restoration committed.
At Stunning Dentistry
The three-gate approval protocol is the single feature UK patients most often tell us they did not receive in prior consultations. High-street cosmetic clinics frequently go from photograph to final crown in two visits. That compression is what produces the 18-month failure cases we see in the chair. Three gates adds two appointments to the timeline. Those two appointments are the reason SD-FMR-05 cases age to ten years without the fracture-and-remake cycle.
Want a personalised treatment plan?
Materials Used for the Definitive Rehabilitation
Material selection in FMR is not a preference, it is an engineering decision driven by location in the arch, opposing dentition, bite force, aesthetic demand, and periodontal status.
Monolithic Zirconia
- 3Y-TZP (3 mol per cent yttria-stabilised tetragonal zirconia polycrystal), highest strength at around 1,200 MPa flexural; moderate translucency; preferred for implant-borne full-arch frameworks and high-load posterior crowns.
- 4Y-TZP multilayer, 900 MPa flexural strength, improved translucency versus 3Y, multilayer blocks replicate natural tooth colour gradation. Our standard for All-on-4 and All-on-6 definitive prostheses.
- 5Y-TZP, 600 to 700 MPa flexural; highest translucency in the zirconia family; appropriate for anterior single crowns and veneers where aesthetics dominate.
Lithium Disilicate (IPS e.max, Vita Suprinity)
PFM (Porcelain-Fused-to-Metal)
CAD-CAM PMMA
PEKK and Pekkton
Polyether ketone ketone. High-performance polymer with flexural strength around 200 MPa and a modulus close to bone, useful as an implant framework substructure where stress distribution matters more than surface hardness. Particularly valuable in zygomatic hybrids where rigidity mismatch can stress the zygomatic attachment.
At Stunning Dentistry
Every FMR prescription names the specific material and grade per unit: "UR6 4Y-TZP multilayer zirconia, UR5 IPS e.max Press, UR4 5Y-TZP layered zirconia." Generic "zirconia" is not a material specification; it is a placeholder. If your UK specialist quote does not name the zirconia grade and the ceramic brand, the quote is incomplete.
Questions about this procedure?

The Evidence Base for Full Mouth Rehabilitation
FMR sits on a body of peer-reviewed evidence that spans occlusal theory, implant survival, prosthetic longevity, and patient-reported outcomes. The references list at the end of this page cites the full set. Here is the shape of the evidence you should know about.
Wear indices, Bartlett and colleagues' 2008 BEWE and Tucker's 2018 consensus provide the scoring backbone for wear quantification. Both are used in every Stunning Dentistry FMR diagnostic file.
At Stunning Dentistry
We measure our own cases against the published literature. Our internal audit, updated quarterly, compares our implant survival, prosthetic survival, and OHIP-14 improvement against the Pjetursson, Abduo, and global benchmark figures. If our numbers ever fall below the published benchmarks, the audit drives the clinical response, not the marketing copy.
Ready to discuss your options?
Candidacy, Medical, Dental, Psychological
FMR candidacy rests on three pillars: medical fitness for the surgical and anaesthetic demands; dental and biological capacity to carry the restoration; and psychological readiness for the multi-phase journey.
Medical Fitness
- Diabetes mellitus, HbA1c below 8 per cent is our threshold for elective surgical phases. Above that, glycaemic optimisation is sequenced before any implant work.
- Anticoagulation, warfarin, DOACs, antiplatelet agents all require pre-surgical review with the patient's prescribing physician. We do not reflexively stop anticoagulation; we plan the surgery within the patient's ongoing regimen where possible.
- Bisphosphonates and osteoporosis medications, oral bisphosphonates under five years of exposure carry a low MRONJ risk; IV bisphosphonates or longer-duration oral exposure requires detailed risk assessment. Denosumab requires particular attention.
- Immunosuppression, any systemic immunosuppressive therapy requires case-by-case assessment, with prosthodontic and surgical input weighed against the indication for the suppressive regimen.
- Cardiovascular status, recent myocardial infarction, unstable angina, or uncontrolled hypertension defer elective work until stabilised.
Dental and Biological Capacity
- Adequate bone volume for the planned implant design (or honest acceptance of grafting or alternative modality if bone is insufficient).
- Periodontally stable residual dentition (or periodontal resolution before any restorative step).
- Opposing arch with a defined plan, a rehabilitated upper arch against a failing lower arch will fail.
- Manageable parafunction, measurable bruxism without uncontrolled psychogenic drivers.
Psychological Readiness
- Realistic expectations about timeline (eight to eighteen months for most FMR cases).
- Acceptance of the multi-trip reality for international patients.
- Commitment to lifetime maintenance, night guard, three-monthly to six-monthly hygienist visits, annual review.
- Absence of active body-dysmorphic presentations. We refer where psychological factors are the dominant driver.
At Stunning Dentistry
Our published FMR decline rate is 11 per cent. That is the share of prospective FMR patients whose diagnostic workup returns a recommendation against proceeding, or in favour of a lower-scope alternative. That figure is not marketing; it is an audit number. A clinic that takes every case is not running a candidacy filter. We run one.
Curious about costs and timelines?
Full Mouth Rehabilitation Modalities Compared
Here is the five-modality comparison table. Use it to orient your thinking; the specific modality for your case is determined in the diagnostic phase.
How to Read This Table
- If cost is the overriding constraint and function can be compromised: conventional complete denture is the fallback. It works; it is not ideal.
- If bone is limited and budget is mid-range: implant overdenture provides meaningful stability with modest implant count.
- If bone permits and you want fixed teeth: All-on-4 or All-on-6 is the standard answer, and the downstream pages walk through each in depth.
- If the dentition is largely preservable and the wear has driven the case: tooth-supported 28-unit rehabilitation is often the biologically preferable choice.
- If the maxilla has resorbed beyond conventional or tilted placement: zygomatic is the answer; for the full clinical detail see the zygomatic page.
At Stunning Dentistry
We run all five modalities in one governance structure. The table above is not a menu. It is a decision framework that leads to a specific recommendation after your CBCT, scans, periodontal chart, and bite analysis are complete.
| Factor | Conventional Complete Denture | Implant Overdenture | Full-Arch Fixed Implant (All-on-4/6) | Tooth-Supported 28-Unit Rehabilitation | Zygomatic Implant Full Arch |
|---|---|---|---|---|---|
| **Lifespan** | 5–7 years before reline/remake | 10–15 years with attachment service | 15–20+ years with maintenance | 15–25 years with maintenance | 15–20+ years with maintenance |
| **Cost (UK private specialist, GBP per arch)** | £1,200–£2,500 | £6,500–£14,000 | £18,000–£28,000 | £14,000–£30,000 | £24,000–£42,500 |
| **Maintenance burden** | Moderate, daily removal, reline every 2–3 years | Moderate, attachment wear, annual service | Low–moderate, hygiene, night guard, annual review | Moderate, hygiene, night guard, unit replacement cycle | Low–moderate, hygiene, night guard, annual review |
| **Aesthetic ceiling** | Adequate | Good | High | Very high | High |
| **Candidacy** | Universal fallback | Two to four implants placeable | Adequate or tiltable bone | Preservable dentition, healthy perio | Severe maxillary atrophy only |
| **Visits / trips** | 4–6 visits | 5–8 visits, 2 trips for overseas | 8–12 visits, 2–3 trips for overseas | 10–18 visits, 2–4 trips for overseas | 8–14 visits, 2–3 trips for overseas |
| **Invasiveness** | Non-surgical | Minor surgical | Moderate surgical | Non-surgical (tooth preparation only) | Major surgical |
| **Reversibility** | Fully reversible | Partially reversible | Non-reversible (implants placed) | Largely non-reversible (tooth structure removed) | Non-reversible |
| **Parafunction tolerance** | Low | Moderate | High | High with correct material | High |
| **Warranty (SD)** | 5 years on prosthesis | 10 years on implants, 5 on prosthesis | Lifetime on implants, 10 years on prosthesis | 10 years on units | Lifetime on implants, 10 years on prosthesis |
Want a personalised treatment plan?
The FMR Journey by Case Complexity, Three Tiers
Not every FMR carries the same scope. We stratify cases into three complexity tiers for scheduling, cost banding, and clinical oversight.
Tier 1, Single-Arch, Single-Modality
- Typical timeline: 6–9 months
- Trips to India: 2
- Total in-clinic time: 14–21 days
- Cost band at Stunning Dentistry: £7,500–£16,000
- Specialist team: prosthodontist + oral surgeon + lab technician
- Example patient profile: a fifty-year-old with upper All-on-4 needed, lower arch intact.
Tier 2, Dual-Arch or Mixed-Modality
- Typical timeline: 8–14 months
- Trips to India: 2–3
- Total in-clinic time: 21–35 days
- Cost band at Stunning Dentistry: £13,500–£28,000
- Specialist team: prosthodontist + periodontist + oral surgeon + lab technician + selective endodontic or TMJ input
- Example patient profile: Graham's staged upper All-on-4 plus lower tooth-supported rehabilitation over fourteen months.
Tier 3, Complex Multi-Discipline
Both arches, multiple modalities, substantial preparation phase (orthodontic intrusion, periodontal regeneration, multiple extractions, bone grafting, or zygomatic placement). Significant aesthetic demand. Parafunction or TMJ component.
- Typical timeline: 12–18 months
- Trips to India: 3–4
- Total in-clinic time: 35–50 days
- Cost band at Stunning Dentistry: £20,000–£42,000
- Specialist team: prosthodontist + periodontist + oral surgeon + orthodontist + TMJ specialist + endodontist + lab technician
- Example patient profile: Alistair's staged orthodontic intrusion followed by bilateral restorative rehabilitation for congenital hypodontia.
At Stunning Dentistry
The tier is determined at the diagnostic workup and drives the scheduling template your CRM manager will build with you. Tier 1 cases are done in two trips; Tier 3 cases need four. We will not compress a Tier 3 case into a Tier 1 schedule because flying is inconvenient. The compression is where long-term failures originate.
Questions about this procedure?
What Determines the Cost of Full Mouth Rehabilitation
FMR cost is driven by six variables. We publish the variables so the quote makes sense.
1. Scope
2. Modality Mix
3. Preparation Phase
4. Material Specification
5. Specialist Team Composition
6. Digital Workflow Intensity
In-house CBCT, intraoral scanning, virtual articulator, CAD-CAM, 3D printing, chairside milling, complete in-house workflow reduces per-unit costs compared to outsourced lab work, which is part of why our pricing is structurally lower.
Ready to discuss your options?
UK Specialist Quotes vs Stunning Dentistry Pricing
We publish these ranges rather than hide them. They are bands, not quotes, your exact figure is finalised after CBCT and prosthodontic consultation.
What the UK GBP figure typically reflects: Harley Street or regional specialist practice overhead, UK laboratory costs, UK compliance and insurance, premium implant systems. NHS does not cover full-arch implant rehabilitation. Private dental insurance (Bupa, AXA, Vitality, Aviva) typically caps at £1,500 to £2,500 per year of dental cover, marginal against a £35,000 figure. Some policies will pre-authorise specialist restorative work at higher limits under specific clinical justification, pathway covered in the next section.
These bands are current as of April 2026 and reviewed quarterly. If the numbers have shifted when you read this, our consultation team will walk you through the current position. We do not operate "today-only" discounts.
| Treatment | UK Private Specialist (GBP) | Stunning Dentistry India (GBP equivalent) | Typical Saving |
|---|---|---|---|
| All-on-4 full-arch fixed, single arch | £18,000–£28,000 | £7,500–£11,500 | £10,500–£16,500 |
| All-on-4 full-arch fixed, both arches | £35,000–£55,000 | £13,500–£20,000 | £21,500–£35,000 |
| All-on-6 full-arch fixed, both arches | £42,000–£62,000 | £16,500–£25,000 | £25,500–£37,000 |
| Full-mouth zygomatic, both arches | £48,000–£85,000 | £18,000–£30,000 | £30,000–£55,000 |
| Full-mouth tooth-supported 28 units (e.max / 4Y-TZP) | £28,000–£60,000 | £7,500–£14,000 | £20,500–£46,000 |
| Staged orthodontic plus restorative FMR | £22,000–£48,000 | £9,000–£17,500 | £13,000–£30,500 |
| Implant overdenture, upper plus lower | £13,000–£22,000 | £6,500–£12,000 | £6,500–£10,000 |
Curious about costs and timelines?
NHS vs Private vs Overseas, The UK Pathway Matrix
The NHS/private question is the first one most UK patients ask. Here is the honest answer.
The Practical Reality
- NHS Band 3 (£319.10 as of April 2025) will cover a conventional denture or a crown where there is documented clinical necessity. It will not cover implant-supported rehabilitation, aesthetic FMR, or specialist multi-discipline restorative work.
- Private UK specialist quotes for genuine FMR sit in the ranges above. "I'd priced a full makeover at a Harley Street specialist, seventy-three grand was their opening figure" is a genuine UK patient quote we hear regularly.
- Private dental insurance, Bupa, AXA, Vitality, Aviva, typically carries an annual cap of £1,500 to £2,500 for most dental cover lines. Pre-authorisation for specialist restorative work is available on some plans with clinical justification, and the pre-auth form requires an itemised quote naming procedure codes, materials, and specialist credentials. We provide every international patient with an itemised invoice suitable for UK insurance reimbursement submission.
- Stunning Dentistry India is not a replacement for NHS care; it is an alternative to UK private specialist care for patients whose clinical need exceeds NHS scope and whose budget is constrained by UK private pricing.
At Stunning Dentistry
We provide every UK patient with an itemised, procedure-coded invoice suitable for submission to Bupa, AXA, Vitality, Aviva, or any other private dental insurer. Our international patient team coordinates with UK insurers on the pre-auth forms where the policy supports it. Many of our UK patients recover between £1,500 and £3,500 from their private extras after the trip. We do not pretend UK private insurance will cover the whole invoice; we make sure you claim whatever you are entitled to.
| Element | NHS | UK Private Specialist | Stunning Dentistry India |
|---|---|---|---|
| Full-arch fixed implant rehabilitation | Not available | £18,000–£55,000 (single to dual arch) | £7,500–£20,000 (single to dual arch) |
| Zygomatic implants | Not available | £24,000–£42,500 per arch | £9,000–£15,000 per arch |
| Tooth-supported 28-unit rehabilitation | Band 3 (£319.10 as of April 2025) covers conventional clinical necessity only; not aesthetic FMR | £28,000–£60,000 | £7,500–£14,000 |
| Conventional dentures (complete) | Band 3 covers if clinical necessity | £1,200–£2,500 per arch | £600–£1,400 per arch |
| Complex periodontal treatment | Band 2 (£73.50) / Band 3 where justified | £3,000–£7,500 course | £800–£2,500 course |
| Specialist prosthodontic consultation | Not typically available under NHS for elective rehab | £250–£450 initial | £120–£220 initial (offset on treatment) |
| CBCT imaging | Not routinely available | £180–£350 per scan | Included in consultation |
| Three-stage approval gate (digital + PMMA + definitive) | Not available | Variable by clinic | Included (SD-FMR-05) |
| Interdisciplinary specialist team | Partially accessible via referral | Available, fee-per-specialist | Included |
| Lifetime warranty on implants | N/A | Clinic-specific | Yes |
Want a personalised treatment plan?
The Interdisciplinary Team Role Matrix
This matrix maps the seven specialist disciplines against the seventeen phases of a Tier 2 or Tier 3 FMR case. "L" denotes lead responsibility; "C" denotes contributing input; blank denotes not involved.
At Stunning Dentistry
The seven-specialist, seventeen-phase matrix is not a marketing chart; it is the template on which every Tier 2 and Tier 3 FMR case file is structured. Each row has a named clinician per case. Each sign-off has a date. If your UK specialist quote does not identify which specialist owns which phase, you do not yet have a plan; you have a proposal.
| Phase | Prosthodontist | Periodontist | Oral Surgeon | Endodontist | Orthodontist | TMJ Specialist | Lab Technician |
|---|---|---|---|---|---|---|---|
| 1. Initial consultation and case intake | L | C | |||||
| 2. CBCT and imaging review | L | C | C | C | |||
| 3. Periodontal assessment and charting | C | L | |||||
| 4. Functional and occlusal analysis | L | C | |||||
| 5. Aesthetic analysis (DSD) | L | C | |||||
| 6. Treatment plan draft | L | C | C | C | C | C | C |
| 7. Case conference sign-off (SD-FMR-05) | L | L | L | C | C | C | |
| 8. Periodontal therapy phase | C | L | |||||
| 9. Endodontic preservation phase | C | L | |||||
| 10. Orthodontic preparation phase | C | L | |||||
| 11. TMJ splint therapy phase | C | L | |||||
| 12. Surgical phase (extractions, implants) | C | C | L | ||||
| 13. Provisional fabrication and delivery | L | C | L | ||||
| 14. PMMA try-in and patient approval | L | C | |||||
| 15. Definitive fabrication | L | L | |||||
| 16. Definitive delivery and occlusal balancing | L | C | C | C | C | ||
| 17. Maintenance and annual review | L | L | C | C | C |
Questions about this procedure?

Step-by-Step: How Full Mouth Rehabilitation Runs at Stunning Dentistry
Phase 1, Remote Pre-Screening
Before you fly, we review your CBCT (taken in the UK) or photographic documentation, your medical history, and your prior dental records. The purpose is to assess whether FMR is the right scope for your case, which modality mix is likely, and which Stunning Dentistry location fits. This is a free remote consultation and many of our UK prospective patients are advised at this stage that their case is Tier 1 and a shorter two-trip pathway is appropriate, or that an alternative to FMR is more suitable.
Phase 2, Trip 1, Diagnostic and Preparation
Typically ten to fourteen days in India for a Tier 2 case, longer for Tier 3.
- In-clinic CBCT, intraoral scans, facial photographs, bite records, functional records
- Periodontal chart, BEWE scoring, TMJ assessment
- Case conference (SD-FMR-05), the prosthodontist, periodontist, and oral surgeon review and countersign the plan
- Preparation phase begins: periodontal therapy, extractions where required, bone grafting or sinus lift if indicated
- Provisional removable or fixed appliances provided for the inter-trip period
- DSD mock-up reviewed with patient; digital mock-up approval gate (SD-FMR-05 Gate 1)
Phase 3, Inter-Trip Period (Back in UK)
Three to six months. Bone healing, periodontal maturation, orthodontic movement where applicable. Weekly to fortnightly Zoom reviews with the lead prosthodontist. Local UK hygienist visits coordinated through our partner-specialist network. Photo uploads to the clinical portal reviewed by the prosthodontist, not a call centre.
Phase 4, Trip 2, Surgical and Provisional
Seven to fourteen days in India.
- Implant placement (All-on-4, All-on-6, or zygomatic as planned) under specialist oral surgery
- Same-day provisional fixed prosthesis where primary stability supports it
- Immediate post-operative reviews on days 1, 3, and 7
- Discharge home with provisional and full written aftercare protocol
Phase 5, Inter-Trip Period
Three to six months of osseointegration. Weekly Zoom reviews for the first month, then monthly. Local hygienist visit at month 3.
Phase 6, Trip 3, Try-In and Definitive
Seven to ten days in India.
- Final impressions and bite records
- PMMA try-in, patient wears for three to five days in their normal life (SD-FMR-05 Gate 2)
- Definitive prosthesis try-in before cementation or final torque (SD-FMR-05 Gate 3)
- Definitive delivery, occlusal balancing, night guard fabrication
- Written warranty, maintenance schedule, and follow-up plan handed over
- Discharge
Phase 7, Trip 4 (Tier 3 only)
Seven to ten days. Definitive delivery of the second arch or second modality, final occlusal balancing across both arches, comprehensive review.
Phase 8, Long-Term Maintenance
Annual in-clinic or remote review for life. Year 1 CBCT to verify marginal bone levels on any implant-supported component. Three-monthly to six-monthly hygienist visits in the UK through our partner-specialist roster.
At Stunning Dentistry
The phase structure is not cosmetic; it drives the clinical calendar for every FMR patient. Each phase has a named clinician, a defined deliverable, and a patient-visible document. SD-FMR-05 is the SOP that keeps the phases aligned across every location we operate.
Ready to discuss your options?

Aftercare and Long-Term Maintenance
FMR prostheses are engineered systems. Every engineered system requires maintenance.
Mandatory Protocols
- Night guard, required for every FMR patient without exception. Bruxism is the primary mechanical threat to long-term prosthetic survival, and the night guard is the single cheapest insurance policy you can apply.
- Hygiene maintenance, every three to four months for the first year, then every six months for life. Hygiene is coordinated with our UK partner-specialist roster for UK patients.
- Annual radiographic review, panoramic or CBCT imaging at year 1 and every two years thereafter to verify marginal bone levels and implant stability.
- Prosthetic screw torque verification, at year 1 and annually on any implant-supported component, the prosthetic screws are torque-verified under controlled conditions.
- Occlusal review, any change in bite, any fracture, any loosening sensation is reviewed immediately.
What Patients Commonly Get Wrong
- Abandoning the night guard after twelve months because "the teeth feel fine now."
- Substituting soft-bristled home care with aggressive inter-dental tools that damage the emergence profile.
- Missing annual reviews because "there is no pain."
- Using whitening products on zirconia or lithium disilicate definitives, they do not whiten, and the hydrogen peroxide can affect the luting cement on veneered units.
Without Maintenance
At Stunning Dentistry
Every FMR patient is handed a written maintenance schedule at definitive delivery. The schedule names the dates (booked, not suggested) of the Year 1 reviews, the radiographic cadence, the hygienist visit frequency, and the CRM contact route. A maintenance schedule suggested in general terms is not a maintenance schedule; it is a disclaimer.
Curious about costs and timelines?
Myths vs Clinical Reality
** A full mouth rehabilitation is basically cosmetic work, crowns and veneers.
** Cosmetic is one output of four. Function, structure, and occlusion are the other three, and they drive the plan. The definition of FMR is the redesign of the bite, not the refinishing of the smile.
** The NHS will do most of it on Band 3.
** The NHS Band 3 (£319.10 as of April 2025) covers specific clinically necessary work, typically a conventional denture or a single crown, not implant-supported full-arch rehabilitation, not 28-unit tooth-supported reconstruction, not aesthetic FMR. Implants are not available under the NHS at any band for elective rehabilitation.
** All-on-4 is a cheaper compromise; All-on-6 is always better.
** All-on-4 is the most widely validated full-arch protocol in the world. For appropriate candidates it is biomechanically adequate and carries 94 to 98 per cent ten-year survival. All-on-6 is biomechanically preferable in high-load or large-arch candidates. The decision is anatomy-driven, not hierarchy-driven.
** My private dental insurance will cover most of the cost.
** Most UK private dental policies cap at £1,500 to £2,500 per year. Some support pre-authorisation for specialist restorative work at higher limits with clinical justification. Either way, private insurance is a partial offset, not a primary funding source for FMR.
** Zirconia does not need a night guard, it is too strong to break.
** Zirconia frameworks fracture less often than layered ceramics, but the screws that retain them loosen, the implants underneath them accumulate stress, and the opposing dentition wears faster without a guard. The night guard protects the system, not just the ceramic.
** If I fly to India, the quality must be lower than Harley Street.
** Quality is a function of specialist training, digital infrastructure, material grade, and protocol compliance, not postcode. Our clinical protocols, implants, and materials are identical to those used on Harley Street. What differs is the cost structure of the overhead.
** The treatment is done in one trip.
** Genuine FMR is two to four trips over 8 to 18 months for international patients. A one-trip "full mouth makeover" is almost always a cosmetic rebuild without the occlusal engineering, the cases that fail at eighteen months.
At Stunning Dentistry
If a clinic tells you an FMR can be done in one trip, in two weeks, in three visits, we would ask them to publish their ten-year survival data. The one-trip full-arch cases are the ones in our audit that come back for remake at five to seven years.
Want a personalised treatment plan?

People Also Ask
What exactly is a full mouth rehabilitation?
Contact your CRM manager immediately. Triage is within 24 hours by Zoom. Routine issues are managed remotely; urgent issues are referred to our UK partner-specialist roster for in-person assessment; emergencies are managed through expedited return to India under the warranty schedule.
Questions about this procedure?
Ask Your Doctor, 12 Questions for Your Consultation
Whether you consult with us, a UK private specialist, or any clinic offering FMR, these are the questions a good doctor will welcome. If any are deflected, you have learned something important.
1. Are you on the GDC Specialist List for Prosthodontics (or the relevant surgical list) for this case?
The General Dental Council Specialist List is the formal UK register. A consultant prosthodontist leading an FMR case should be on the Prosthodontics list; surgical components should be led by clinicians on the Oral Surgery or Periodontics lists. Ask for the registration number; verify it at gdc-uk.org.
2. How many GDC-registered specialists will personally touch my case?
A genuine Tier 2 or Tier 3 FMR case needs at least three specialists across prosthodontics, periodontics, and oral surgery. A case led solo by a General Dental Practitioner is a flag for any multi-modality FMR.
3. Can the NHS do any part of this?
The honest answer is usually no for implant-supported or aesthetic FMR. Some components, a periodontal course of treatment, a clinically necessary denture, may fall within NHS scope at Band 2 or Band 3. Any clinician should give you a clear NHS-versus-private breakdown before you commit.
4. Which implant system will you use, and why that system?
Nobel Biocare and Straumann are the two systems with the longest and deepest published ten-year-plus data. Osstem, Dentsply, and Zimmer are reasonable alternatives with shorter or narrower datasets. Any brand not on an international-certification tier is a flag.
5. What materials will be used for the definitive, and what grade?
"Zirconia" is not a specification. Ask for the grade (3Y-TZP, 4Y-TZP multilayer, 5Y-TZP) per unit, and the ceramic brand for any aesthetic-led layering (IPS e.max, Vita Suprinity, layered zirconia blocks). If the quote does not name the grade, the quote is incomplete.
6. What is the written warranty, on implants, on prosthesis, on labour, and what is the claim process?
Get it in writing. Ask specifically what is covered, what is excluded, for how long, and what happens if you are across the world when something fails.
7. What is your complication rate and your revision protocol?
Published mechanical complication rates for FMR components sit at 20 to 35 per cent over long-term follow-up. A clinician claiming zero complications is not being honest. Ask the specific figure for their practice and how they handle screw loosening, veneer chipping, and peri-implantitis.
8. What if a tooth or implant fails mid-treatment?
The honest answer involves who pays, who decides on the replacement modality, and how the timeline adjusts. Any clinic without a clear written policy is a flag.
9. What is your splint therapy protocol and how does it sequence with the restorative work?
A proper FMR includes splint therapy as a diagnostic tool (pre-treatment) and as a protective tool (post-treatment lifelong). If the plan does not include a named splint at both stages, the plan is incomplete.
10. How many trips will I need and over what timeline?
Two to four trips over 8 to 18 months is the honest range for international FMR. A one-trip promise is the most common warning sign of an underspec'd plan.
11. What is your refurbishment and remake policy?
Beyond the warranty terms, what happens at year 12 or year 15 if a unit fractures? Is there a discount on remake for loyal patients? Is there a policy at all?
12. What is your post-treatment support pathway if I have a problem while in the UK?
For overseas clinics, this is the most critical question. Ask about the CRM response time, the UK partner-specialist roster for urgent in-person care, the emergency return-travel policy, and the named escalation point. Answers that are vague are disqualifying.
*Print this section. Bring it to your consultation. If a clinic, including ours, cannot answer these twelve questions clearly and in writing, it is not the right clinic, regardless of price.*
At Stunning Dentistry
We have watched UK patients use this exact list to choose a different clinic. We are entirely comfortable with that. Some of those patients have had excellent outcomes elsewhere because the list exposed the right questions. A patient who chooses another clinic because our answers did not satisfy them is a patient who will choose their next clinic more carefully too. The list serves the patient, not us.
Ready to discuss your options?

Full Mouth Rehabilitation at Stunning Dentistry
Clinical Infrastructure
- Over twenty surgical operatories across our Hyderabad flagship and partner locations
- Complete in-house digital workflow: CBCT, 3Shape TRIOS and Medit i700 intraoral scanning, Zirkonzahn PlanOral virtual articulator, 3Shape Dental System and exocad CAD, Roland DG Shape and Imes-Icore milling, Formlabs 3D printing, dedicated zirconia sintering rooms
- Hospital-grade sterilisation: single-use materials where applicable, HEPA air filtration, multi-layer sterilisation protocols aligned with international standards
Clinical Governance
- Every FMR case planned and countersigned under SD-FMR-05 by Dr. Priyank Sethi and a senior consultant prosthodontist
- Three-stage patient approval gate on every FMR: digital mock-up, PMMA try-in, definitive
- Weekly case conference reviewing every active multi-modality plan
- Accredited with AAID, AACD, AAO, and BACD
- Internal audit cycle quarterly: implant survival, prosthetic survival, OHIP-14 score change, complication rates
The Commitment
- Lifetime warranty on Nobel Biocare and Straumann implants under normal use
- Ten-year documented warranty on definitive zirconia prosthesis
- 24/7/365 dedicated CRM support across all patient touchpoints
- International patient services: visa coordination, flight planning, hotel partnerships, airport transfers, translator support
At Stunning Dentistry
The infrastructure list is not inventory; it is the operating manual of a single-specialty dental hospital. CBCT, milling unit, sintering oven, sterilisation suite, and operatories are under one building, one governance, one accountability chain. That is what a specialist centre looks like when it is engineered from the ground up.
Curious about costs and timelines?
For UK Patients: Your Journey to India
We have built a structured pathway for UK patients, not an improvisation. FMR consolidates a case that would take eighteen months of serial visits at home into two, three, or four concentrated trips. The clinical protocol is identical to what you would receive on Harley Street or in Edinburgh; what changes is the cost structure, the specialist bench depth, and the in-house digital infrastructure.
The Multi-Trip Model
- Full diagnostic workup: CBCT, intraoral scans, photographs, periodontal chart, BEWE scoring, functional records, TMJ assessment
- SD-FMR-05 case conference and patient approval gate 1 (digital mock-up)
- Preparation phase where required: periodontal therapy, extractions, bone grafting, sinus augmentation, or initial orthodontic placement
- Provisional appliances fitted for the inter-trip period
- Discharge home with written inter-trip protocol and CRM contact
- Implant placement (All-on-4, All-on-6, zygomatic as planned)
- Same-day provisional fixed prosthesis where primary stability supports it
- Post-operative review at days 1, 3, 5, and 7
- Hygiene training session
- Discharge home with provisional and SD-FMR-05 inter-trip protocol
- Final impressions and bite records
- PMMA try-in worn for three to five days (patient approval gate 2)
- Definitive prosthesis try-in before commitment (patient approval gate 3)
- Definitive delivery and occlusal balancing
- Night guard fitting
- Written warranty, maintenance schedule, and follow-up plan handed over
- Definitive delivery of the second arch where staged
- Final occlusal balancing across both arches
- Comprehensive one-year plan review
What We Coordinate for You
- India medical e-visa guidance (typically issued within 72 hours of application)
- Flight booking guidance through vetted partners, direct routes from Heathrow, Manchester, Gatwick, Birmingham, and Edinburgh to Mumbai, Delhi, Hyderabad, and Bangalore (9 to 10 hours direct)
- Hotel partnership rates at 4-star properties within 10 to 20 minutes of the clinic
- Airport pick-up and drop-off included
- Dedicated CRM manager assigned before first booking, available 24/7/365
- Translator support where required (most clinical staff are fluent English speakers)
Companion Travel
We strongly recommend a travelling companion for Trip 2, a partner, family member, or friend. Post-surgical recovery is straightforward but having one trusted person with you is part of the protocol, not an extra. Companion accommodation is shared at the same hotel; companion airport transfers are included.
UK Insurance Reimbursement Pathway
- Itemised, procedure-coded invoices issued for every treatment phase
- Pre-authorisation forms for Bupa, AXA, Vitality, Aviva, and other UK dental insurers prepared on request before the trip
- Clinical narrative letters from the lead prosthodontist to support the pre-auth submission
- Post-treatment claim documentation emailed in UK-standard format for reimbursement submission
- Typical UK insurance recovery: £1,500 to £3,500 per patient depending on policy and scope
At Stunning Dentistry
The UK journey is not a travel package with a dental appointment bolted onto it. It is a clinical pathway engineered against SD-FMR-05, with travel logistics coordinated around the clinical calendar. Dental tourism fails at handoffs. We engineer improvisation out.
Want a personalised treatment plan?

What This Costs in GBP, Your Out-of-Pocket Reality
Here is the full out-of-pocket figure for a UK patient, not just the clinical fee.
Tier 1, Single-Arch All-on-4 (Zirconia Definitive)
Tier 2, Dual-Arch All-on-4 (Zirconia, Full Mouth)
Tier 3, Complex Multi-Modality (Orthodontic + Restorative Both Arches)
What Private Insurance and NHS Cover
- NHS: Band 3 (£319.10 as of April 2025) for clinically necessary components only; implant-supported FMR is not available under the NHS.
- UK private dental insurance: Bupa, AXA, Vitality, Aviva, and similar typically cap annual dental cover at £1,500 to £2,500. Pre-authorisation for specialist restorative work is available on some plans with clinical justification.
- At Stunning Dentistry: itemised procedure-coded invoices for UK insurance submission; typical UK insurer recovery £1,500 to £3,500.
Cost figures current as of April 2026 and reviewed quarterly.
At Stunning Dentistry
The only comparison that matters is total-to-total, not clinical-fee to clinical-fee. If the total UK out-of-pocket for flying is under the UK private clinical fee by less than £8,000 to £10,000, we will tell you the flight is probably not worth it. Transparency over persuasion.
| Line Item | GBP Range |
|---|---|
| Clinical fee at Stunning Dentistry | £9,000–£17,500 |
| Return flights (three to four return trips) | £1,300–£2,200 |
| Hotel accommodation (35–50 nights total) | £1,400–£2,500 |
| Visa, insurance, ground transport | £250–£450 |
| Companion travel | £900–£1,600 |
| **Total UK out-of-pocket, Tier 3** | **£12,850–£24,250** |
| Equivalent quote at UK private specialist | **£22,000–£48,000** |
| **Net saving** | **£9,150–£23,750** |
Questions about this procedure?

Is This Worth Flying For? The Decision Framework
When India Is Clearly the Right Call
- UK private specialist quote exceeds £22,000 and savings after all travel costs exceed £8,000
- You are medically fit for international travel (no active anticoagulation crisis, no recent cardiac event within 6 months, HbA1c under 8 per cent)
- You can commit to two to four trips over 8 to 18 months, with return visits spaced by 3 to 6 months
- You are comfortable with structured remote follow-up between visits via Zoom and our UK partner-specialist roster
- You want access to in-house CBCT, CAD/CAM, 3D printing, and a consultant-led specialist team without UK private-specialist overhead
When India Is Not the Right Call
- Single-tooth or single-unit work where UK price differential is modest and travel cost erases the saving
- Active health issues contraindicating international travel
- Inability to commit to the remote-follow-up model
- An existing UK specialist relationship you do not wish to interrupt
- Savings under £5,000 after honest accounting
When to Get a Second Opinion First
- Pressure to commit on the day of first consultation, whether in the UK or in India
- Any quote for FMR that has not seen your CBCT
- Any quote under £5,000 per arch that claims full-arch implant rehabilitation with branded implants (verify)
- Any plan that does not name the implant system, the zirconia grade, and the specialist team by GDC or equivalent registration
We offer free remote CBCT-based assessment for UK patients before you commit to flying. A meaningful proportion of those assessments conclude that the UK option is right for the case. No fee applies.
At Stunning Dentistry
We run 40 to 60 free remote consultations per month for UK patients. A non-trivial share are advised to stay in the UK because the case is Tier 1 small-scope, because the UK private quote happens to be at the lower end, or because the patient's medical profile makes international travel risky. Trust earned beats booking earned, every time.
Ready to discuss your options?
Pre-Travel Checklist for UK Patients
8 Weeks Before Trip 1
- Submit your existing CBCT or panoramic radiograph for remote pre-screening (or we arrange one at a UK partner radiology centre)
- Complete medical history form
- Confirm fitness to travel with your UK GP, written clearance preferred for any complex medical history
- Apply for India e-medical visa (allow 5 working days for processing)
- Book flights, ensure the return date is at least day 10 after the surgical trip
- Notify your UK private dental insurer of planned overseas treatment and request pre-auth forms
4 Weeks Before Trip 1
- Confirm hotel booking via our partner network
- Arrange travel insurance with international medical cover and treatment-interruption protection
- Finalise deposit or staged payment per the booking schedule
- Confirm companion travel arrangements
- Refill prescriptions for the trip duration
- Book your GP visit closest to departure for any final clearance documents
1 Week Before Trip 1
- Confirm airport pickup with your CRM manager
- Pack soft foods, protein shakes, and any familiar-brand supplements for the first post-op trip (some are easier from the UK than to source locally)
- Pack your existing night guard if you have one
- Print treatment plan, pre-authorisation letters, warranty provisions, and emergency contact card
- Notify your bank of international travel
- Confirm SIM or eSIM for India, a working phone is safety-critical
Day Before Departure
- Light meals only if you have any reflux concerns
- Pack medications in carry-on, not checked luggage
- Confirm pickup time, hotel address, and CRM manager phone number in your phone
At Stunning Dentistry
This checklist was refined case by case across hundreds of UK patients. Every item on the list is here because someone arrived without it once. The visa timing item exists because of a 2022 Manchester patient whose visa came through on the morning of departure. The SIM item exists because of a 2023 Leeds patient who landed without data and could not reach the driver. Engineered, not templated.
Curious about costs and timelines?
Your Time in India, Multi-Trip Schedule
A real schedule for a real trip, based on the UK FMR patients we treat regularly.
Trip 1, Diagnostic and Preparation (Example: 12-Day Visit)
Inter-Trip Period (At Home in the UK, 3–6 Months)
- Week 1: Zoom review, photo upload to clinical portal
- Weeks 2–4: Fortnightly Zoom reviews
- Months 2–3: Monthly Zoom reviews; UK hygienist visit through partner-specialist roster
- Months 4–6: Pre-Trip 2 briefing; booking confirmation for Trip 2
- Direct CRM access throughout, response within 4 hours business, 24 hours overnight
Trip 2, Surgical and Immediate Loading (Example: 10-Day Visit)
Trip 3, Try-In and Definitive (Example: 8-Day Visit)
At Stunning Dentistry
Trip 1 is twelve days by design: six days of clinical work, six days of rest and observation. Trip 2 is ten days: three post-op review days built in for safety, not as a marketing amenity. Trip 3 compresses to eight because the fabrication runs in our laboratory while you rest. The schedule is engineered for clinical outcomes, not to match marketing imagery.
| Day | What Happens |
|---|---|
| Day 1 | Arrival, rest |
| Day 2 | Final impressions, scans, occlusal records |
| Day 3 | Free day while definitive is fabricated |
| Day 4 | PMMA try-in (patient approval gate 2); patient wears PMMA for 72 hours |
| Day 5 | Rest and adaptation to PMMA |
| Day 6 | PMMA review, definitive try-in (patient approval gate 3), definitive delivery, occlusal balancing |
| Day 7 | Night guard fitting, warranty and maintenance schedule, final review |
| Day 8 | Departure |
Want a personalised treatment plan?
Back in the UK, Your Follow-Up Plan
The work is not finished when you board the return flight. Long-term success is built in the months and years that follow.
Year 1, The High-Vigilance Year
Year 2 Onwards
- Annual remote review by Zoom, clinical photos, hygiene photos, radiograph upload
- Annual UK hygienist visit through our partner-specialist roster
- Optional in-person review at Stunning Dentistry every 2 to 3 years
- Lifetime warranty active throughout
Our UK Partner-Specialist Network
What "Remote" Actually Means
Not a substitute for in-person care, a structured complement. Your Zoom consultation is with the same consultant prosthodontist who treated you, or their named deputy. Photos are reviewed by the clinical team, not a triage algorithm. If anything is unclear or concerning, you are escalated to a UK partner-specialist for in-person review immediately.
At Stunning Dentistry
The UK follow-up calendar is booked into the lead prosthodontist's clinical calendar alongside their in-person Indian cases. A UK patient's Zoom review is not a separate "international division" appointment; it is in the same calendar. Year-one follow-up is a clinical responsibility, not a courtesy.
| Timepoint | What Happens | Where |
|---|---|---|
| Week 1 home | Zoom check-in, hygiene photo review, healing assessment | Remote |
| Month 1 | Zoom consultation, prosthodontist review of intraoral photos | Remote |
| Month 3 | Zoom consultation + UK hygienist visit through partner-specialist roster | Remote + UK |
| Month 6 | Zoom consultation, radiograph review (you upload a panoramic taken in UK, we cover the cost up to £250) | Remote |
| Month 12 | First annual review, Zoom consultation, CBCT upload, comprehensive clinical photo review | Remote |
Questions about this procedure?
If Something Goes Wrong After You're Home
No full-arch reconstruction is risk-free, and you are 7,500 km from the clinic. Here is the protocol, written so that if you need it, you know exactly what to do.
Step 1, Contact Your CRM Manager Immediately
- Single point of contact, 24/7/365
- Phone, email, or WhatsApp
- Response time: under 30 minutes business hours, under 4 hours overnight
Step 2, Triage Within 24 Hours
- Same-day or next-day Zoom consultation with your prosthodontist
- Photo and intraoral video review
- Initial assessment: routine, urgent, or emergency
Step 3, Escalation Pathway
- Routine issues (loose component, hygiene concern): managed remotely, addressed at next planned visit
- Urgent issues (persistent pain, suspected infection, screw failure): referral to our UK partner-specialist roster for in-person assessment, with full clinical records shared, and the visit reimbursable under warranty terms where qualifying
- Emergencies (acute infection, major prosthetic fracture, suspected implant failure): immediate in-person assessment in the UK, and expedited return travel to Stunning Dentistry for definitive management, with flights and accommodation supported per the warranty schedule
NHS Emergency Pathway
- NHS 111 for non-emergency urgent dental advice (in-hours or out-of-hours)
- 999 or A&E for life-threatening emergencies, severe facial swelling compromising airway, severe post-operative bleeding, suspected systemic infection
- Emergency dental services are available through NHS 111 routing; our CRM team will advise you through the call if needed
GDC Complaints and Regulatory Pathway
- Our clinicians hold equivalent specialist certifications; if you have a formal complaint, our internal pathway is documented in the warranty schedule
- For any UK-based care delivered under our partner-specialist roster, the GDC complaints pathway (gdc-uk.org) is the formal UK route
- We will cooperate fully with any GDC review concerning a UK partner clinician whose care is connected to a Stunning Dentistry case
Warranty Coverage in Plain Language
- Implants: lifetime warranty on Nobel Biocare and Straumann against failure to integrate or premature loss (excluding wilful neglect or trauma)
- Prosthesis: ten-year documented warranty on definitive zirconia against material defects and structural failure under normal use
- Repair fees: waived under warranty terms, only travel costs (in qualifying scenarios) and lab consumables apply
- Documentation: every patient receives the written warranty document at definitive delivery
At Stunning Dentistry
Every component of this emergency protocol exists because across the last ten years we needed it. The UK partner-specialist roster was built case by case after a 2021 Manchester patient needed urgent in-person review at a weekend. The flight-supported revision clause was added after a 2023 Cardiff fracture case. Written by experience, not by marketing.
Ready to discuss your options?
Your Dental Tourism Safety Framework
If you are travelling for dental work, whether to us or to anyone else, these are the warnings to take seriously.
Reject Any Clinic That:
- Quotes a price without seeing your CBCT or reviewing your full medical history
- Guarantees a specific treatment ("All-on-4") before clinical assessment
- Refuses to name the implant brand or the specific zirconia grade they will use
- Cannot show you 10-year published data for the implant system
- Has no published or accessible warranty terms in writing
- Pressures you to commit on the day of inquiry or offers a "today-only" discount
- Cannot tell you the named clinician who will perform the surgery
- Has no in-house CBCT, no in-house CAD/CAM, no in-house lab, and outsources everything
- Does not have a structured remote follow-up protocol for international patients
- Has no recourse pathway if something fails after you return home
- Mixes prices into a single all-inclusive figure that you cannot break down line by line
- Has no independent reviews and no transparent complications data
What a Safe Clinic Looks Like:
- Specialist-led care (named prosthodontist + named oral surgeon + named periodontist)
- Internationally certified implant systems (Straumann, Nobel Biocare, Osstem, Dentsply, Zimmer)
- Hospital-grade sterilisation
- Published clinical outcomes
- Written warranty document
- Structured pre-op, intra-op, and post-op protocols
- Transparent itemised pricing
- A contactable post-op support system in the UK (partner-specialist roster, documented escalation)
- Willingness to tell you when their treatment is not the right fit for you
At Stunning Dentistry
We are entirely comfortable being rejected on our own test. Rather a patient fly to a different clinic and have a great outcome than fly to us because they felt pressured. The safety framework is written to the standard we would apply to a family member.
Curious about costs and timelines?
UK Patient Stories
The patient experiences referenced here are paraphrased from consented patient testimony. Names have been verified; clinical outcomes are accurate.
Graham, 67, Newcastle
Priya, 52, Leeds
Alistair, 48, Edinburgh
Alistair told us at the twelve-month review that the combination of the orthodontic intrusion and the restorative redesign had changed the shape of his face more than he had anticipated, the reopened VDO restored lip support and reduced a perioral wrinkle pattern that he had attributed to ageing alone.
We do not publish patient stories as marketing, we publish them because UK readers asked us to. Every story above is consented, fact-checked against the clinical record, and edited only for privacy. We are happy to put new prospective patients in direct touch with previous UK patients (with their explicit permission) at the consultation stage.
Want a personalised treatment plan?
Partner Dentists in the UK, Our Network Roadmap
Honesty first: as of April 2026, our in-UK partner network is in active expansion. We do not pretend to have a clinic on every high street. Here is exactly where we stand and where we are going.
What Is Live Today
- Remote follow-up, 24/7 CRM, structured Zoom protocol, consultant prosthodontist-led photo and radiograph review, operational now for every UK patient.
- UK hygienist roster, GDC-registered hygienists in London, Manchester, Edinburgh, Birmingham, Leeds, Bristol, Cardiff, Belfast, and Newcastle who provide local maintenance with full clinical-record sharing.
- Emergency referral pathway, confirmed referral relationships with select UK GDC Specialist List prosthodontists, periodontists, and oral surgeons for urgent in-person assessment under our warranty terms.
What Is Building Through 2026
- Formal partner-clinic agreements in London, Manchester, Edinburgh, and Birmingham, clinics where in-person review and routine maintenance can happen as part of an integrated pathway
- Annual in-UK clinical days by a Stunning Dentistry consultant prosthodontist on a rotating basis for patient reviews and prospective consultations
- A published partner-clinic directory with GDC Specialist List credentials, scope of supported services, and patient feedback
What This Means for You
- Full-quality clinical care during your trips
- A structured remote follow-up that works
- A clear emergency pathway in the UK if something goes wrong
- A network roadmap that expands the in-person UK touchpoints throughout the year you are under our care
We will not oversell what does not yet exist. The remote follow-up is operational. The in-person UK footprint is growing. Both will be true on the day you book and both will be stronger six months later.
At Stunning Dentistry
This is a deliberate decision not to fabricate a UK "presence" we do not yet hold. Plenty of dental-tourism operators list partner clinics that turn out to be a phone-forwarding number. Under-promise; outperform.
Questions about this procedure?
Clinics in India, Which Stunning Dentistry Location Fits Your Trip
Stunning Dentistry operates from multiple locations across India, each equipped for full-mouth rehabilitation. The right destination for your trip depends on your UK origin city, your flight preference, and your case complexity.
Our FMR-Capable Locations
What Is the Same Across Every Location
- Consultant prosthodontist-led team under Dr. Priyank Sethi's clinical governance
- Identical CBCT, intraoral scanning, CAD-CAM, and 3D printing infrastructure
- Same Nobel Biocare and Straumann implant systems
- Same SD-FMR-05 protocol and three-gate patient approval
- Same lifetime warranty
- Same 24/7 CRM support pathway
What Differs
- Volume of international patient programmes (Hyderabad runs the largest by volume)
- Availability of zygomatic surgery (Hyderabad flagship only)
- Adjacent travel and recovery options (city character, hotel options, post-op tourism)
- Direct versus one-stop flight options from your UK origin city
How We Help You Choose
At Stunning Dentistry
One clinical governance framework, one SOP library, one warranty, one accountability chain. Implant brand, milling workflow, prosthodontist-to-surgeon pairing, and post-op pathway are identical across Hyderabad, Delhi, Mumbai, and Bangalore. Uniformity is a deliberate engineering choice.
| Location | Access from UK | Suited For |
|---|---|---|
| **Hyderabad, Flagship Hospital** | Direct or 1-stop from Heathrow, Manchester, Gatwick (9–10 hours direct) | All case tiers including Tier 3 zygomatic and complex multi-modality |
| **Delhi NCR** | Direct from Heathrow, Manchester, Birmingham | Tier 1 and Tier 2 cases; patients combining treatment with North India travel |
| **Mumbai** | Direct from Heathrow | Tier 1 and Tier 2 cases; patients combining with West India travel |
| **Bangalore** | 1-stop from Heathrow, Manchester | Tier 1 and Tier 2 cases; patients with family in South India |
Ready to discuss your options?
Clinical References
This article references the following peer-reviewed and consensus literature:
All clinical claims are sourced from indexed peer-reviewed publications or from named UK specialist society guidance. No manufacturer-sponsored data is presented as independent evidence.
Curious about costs and timelines?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
What is the difference between FMR and a smile makeover?
FMR redesigns the bite; a smile makeover refinishes the visible surfaces. The aesthetic output can overlap, but the underlying work is fundamentally different. A smile makeover without occlusal engineering frequently fails mechanically within seven years. An FMR includes the smile makeover as part of the scope, but anchors the aesthetics to a functional design.
Do I need to be on the GDC Specialist List to do FMR in the UK?
The clinician planning your FMR should hold an entry on the GDC Specialist List in Prosthodontics, with the surgical components delivered by specialists in Oral Surgery or Periodontics, depending on scope. General Dental Practitioners can deliver components of FMR, and many do excellent work, but a complex multi-discipline case requires specialist oversight. Always ask to see the GDC Specialist List registration number.
How many implants will I need?
Between zero (tooth-supported rehabilitation) and eight per arch (rare, typically in high-load or zygomatic-hybrid cases). The commonest configurations are four (All-on-4) and six (All-on-6) per arch.
Will my face look different after FMR?
Yes, typically in a more youthful direction. Most FMR cases involve recovering lost vertical dimension of occlusion, which restores lip support, shortens the philtrum, and reduces perioral wrinkling. The structural change is real; it is the restoration of proportion that had been lost as the bite collapsed.
Can I get a second opinion on my treatment plan?
Yes, and we recommend you do. Our SD-FMR-05 protocol includes an internal second opinion by a separate senior prosthodontist. We also welcome external second opinions from UK consultant prosthodontists and can provide our complete digital file (CBCT, scans, DSD mock-up) for that review.
What if I have TMJ problems before starting?
Pre-existing TMJ symptoms are assessed at the initial workup by our TMJ specialist. In most cases, splint therapy is sequenced before any restorative step, often three to six months of stabilisation before irreversible work begins. Ignoring pre-existing TMJ and "fixing the bite to fix the jaw" is a common cause of FMR failure. My GP was actually the one who flagged the jaw pain was TMJ, not anxiety, that is a patient quote we hear regularly.
What is the splint therapy protocol?
A hard acrylic flat-plane stabilisation splint worn at night, and during the day in high-bruxism patients, for a minimum of three months pre-treatment in TMJ-involved cases. Splint adjustment appointments at 2, 4, 8, and 12 weeks. Diagnostic information from the splint (wear patterns, symptom response) feeds directly into the occlusal design.
What is your refurbishment and remake policy?
Lifetime warranty on Nobel Biocare and Straumann implants against failure to integrate (excluding wilful neglect or trauma). Ten-year documented warranty on definitive zirconia prostheses, if the zirconia framework fractures within ten years under normal use, it is remade at no additional laboratory or clinical fee. Refurbishment of veneered porcelain chipping is covered under the first five years; after five years, chipping repair is costed but discounted.
What materials and warranties cover my case?
The exact material specification per unit is published in your treatment plan. The warranty document is handed to you at definitive delivery, in writing, not verbally. You may request a copy in advance of the first trip, many UK patients do, and we provide it as standard.
How many trips and over what timeline?
Tier 1: two trips, six to nine months. Tier 2: two to three trips, eight to fourteen months. Tier 3: three to four trips, twelve to eighteen months. The schedule is built with your CRM manager at the pre-screening stage.
What if a tooth or implant fails mid-treatment?
Failure during osseointegration is rare (under 2 per cent on All-on-4 in our registry) but planned for. A failed implant is replaced at no additional surgical fee under the warranty schedule. A tooth that fails during the preparation phase is addressed through the next-appropriate modality, if extraction-and-implant becomes necessary where tooth preservation was planned, the treatment plan is revised and re-consented.
Can I combine my FMR with any aesthetic work on the face (not just teeth)?
We do not provide non-dental aesthetic work in-house. Some of our UK patients schedule dental-compatible facial aesthetic procedures (facial harmonisation by appropriately licensed practitioners) around their India trips. We can advise on timing relative to the dental sequence but we do not coordinate the non-dental work.
How do I know the specialist-supervised protocol actually happened?
Every SD-FMR-05 plan carries the GDC equivalent registration number of each clinician involved and their signature on the sign-off date. The Tuesday-morning case conference attendance is logged. The three approval gates are signed by you in the clinical record. You receive the full file on request.
What if I do not finish the course?
The treatment plan is structured so every trip ends with a functional and stable interim state. If you cannot return for trip 2 or trip 3 as planned, your interim provisional is serviceable for months. We would strongly advise completing the sequence, but the interim states are designed to be safe, not to force your hand on scheduling.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










